March 14, 2024

Moving Measures to Conversations:

Children and adolescents are experiencing increasing rates of anxiety, depression, and behavior problems.1 Accessing behavioral health treatment can be a challenge, and when children do receive treatment, outcomes are generally modest.2 Efforts to disseminate evidence-based practices (EBPs), or those that have been shown to be more effective than usual care, are increasing and help improve the quality and outcomes of behavioral health services.
Measurement-based care (MBC) is the process of routinely administering and discussing results of assessment measures with youth and their caregivers and using this information to help guide treatment towards achieving youth and family goals.3,4 MBC is an EBP that can be applied to a range of treatment approaches, types, and settings to improve the quality of care for youth, regardless of presenting concern. A key component of MBC is engaging youth and families in using outcome measures to inform treatment and decision making. However, while providers are increasingly implementing MBC and becoming more comfortable using standardized measures to track treatment progress, they may struggle to fully engage youth and families in this process. This issue brief highlights strategies for fully engaging youth and families in MBC in ways that are feasible and helpful for both clinicians and families.
Children show greater improvement when their clinician regularly administers measures and shares the results with them, compared to children whose clinicians do not.5,6 Despite the evidence, MBC is less consistently used with racial or ethnic minorities or families who experience socioeconomic strain.7 This suggests that MBC may not be reaching families equitably and that there are opportunities to improve how MBC is implemented so that youth and caregiver perspectives are consistently represented when evaluating treatment progress and making treatment decisions. Additionally, even when measures are used, they may be selected, administered, and interpreted with little input from youth and families. By ensuring youth and caregiver involvement throughout the MBC process, clinicians can help promote family-centered care, strengthen therapeutic relationships, and reduce disparities in children’s behavioral health access, quality, and outcomes (see Figure 1).
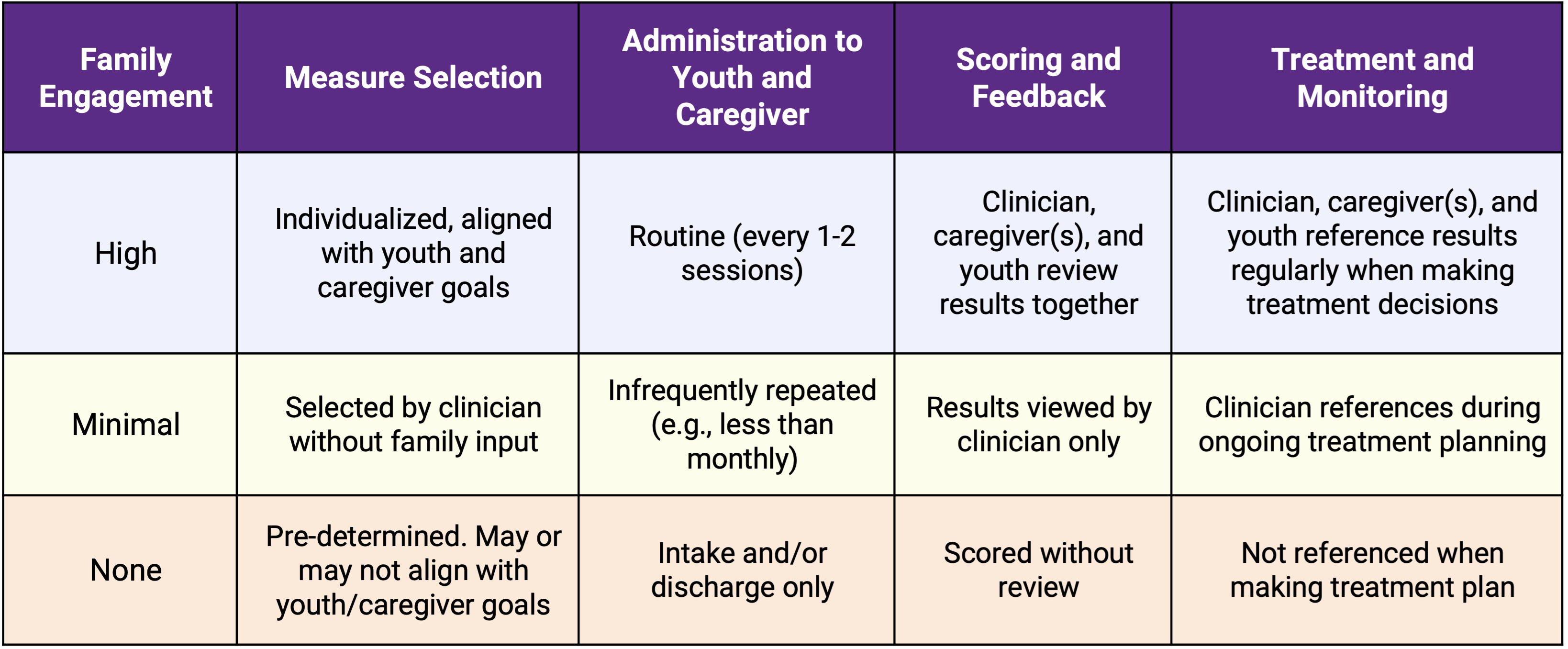
Figure 1. Best Practices for Engaging Youth and Families in MBC
There are two common systemic challenges that can limit true youth- and family-centered MBC in children’s behavioral health:
There are many different types of measures that can be used with youth and their caregivers. However, problematic behaviors and symptoms are among the most common domains assessed in children’s behavioral health, while individualized (or patient-generated) measures are among the least common domains assessed.8,9 Symptom-specific measures are helpful for some families and for giving a system-level, birds-eye view of how well treatments work for common concerns for which youth present to treatment, but they may or may not align with what many families consider their main concerns and treatment goals. In fact, youth tend to identify therapy goals that fall into categories of relationships, coping, and personal growth more often than goals related to specific symptoms.10 While we don’t yet know how individualized measures may help reduce disparities in treatment engagement and outcomes for diverse families in particular, increasing their use has been recommended as one way to improve the fit of MBC with diverse cultural perspectives and to make outcomes more equitable.4
Engaging youth and families in MBC is also naturally tied to how frequently measures are administered and how consistently the results are jointly discussed and interpreted with youth and families. Nationally, only about 5% of clinicians use measures every 1-2 sessions, and fewer than 10% use measures monthly.11 To achieve the best outcomes, measures should be collected and discussed with youth and families during each treatment session.3 National research has also shown that feedback about the results of measures is shared with fewer than half of clients.12 In a recent survey of Connecticut providers, clinicians reported administering standardized measures and discussing outcomes with fewer than 40% of the clients they served in the prior week. Without collaborative, routine progress monitoring, it is harder to assess how well behavioral health services are working for youth and where changes are needed to ensure families receive care that aligns with their values and reasons for seeking treatment.
Many youth-serving clinicians report positive attitudes about the utility and benefit of regularly using measures.13 However, having positive attitudes towards MBC does not necessarily predict its use in practice. Instead, clinicians tend to regularly use measures when they believe 1) doing so is practical in their clinical work and 2) that their organizations support the use of evidence-based practices, including MBC.11,13
In a survey of Connecticut providers, clinicians expressed difficulty using measures due to a range of factors, including:
Efforts to increase youth, family, and clinician engagement with MBC should address these practical barriers for clinicians and families. It is also important to improve our understanding of youth and caregiver preferences in the MBC process and increase transparency with families about why and how measures are used in their child’s treatment.
A recently proposed and promising framework, the Strategic Treatment Assessment with Youth (STAY) model,4 offers guidance for using MBC to help address these barriers, improve collaboration, and reduce disparities in youth behavioral health. STAY may be particularly important for children and families whose perspectives about treatment needs and outcomes have been historically minimized and who have experienced concerns related to confidentiality and mistrust in the American health system. For example, the STAY model emphasizes transparency, therapeutic alliance, acknowledgments of discrimination, and patient-generated measures to promote treatment that is truly youth and family-centered.
MBC that is youth and family-centered must be relevant to youth and family concerns, relevant to treatment, and feasible to implement within the ongoing demands of behavioral health practice.
Clinicians serve a major role in making MBC youth and family–centered. They are best positioned to explain a measure’s purpose, interpret scores with youth and families, and facilitate discussions about preferences for types of progress indicators. Clinicians have also expressed a desire for autonomy in selecting measures to help ensure they are relevant to their clients.14 One way to ensure direct relevance of measures to families and clinicians is by including youth and caregiver-generated metrics in MBC, which focuses progress monitoring on youth and families’ key concerns and treatment goals.4,11 One example of this type of measure is the Top Problems Assessment (TPA), which uses youth and caregiver perspectives to identify and monitor the severity of the most important problems they are experiencing. The TPA can capture improvement during treatment,17 and to date, over 300 clinicians in Connecticut have been trained to use the TPA through the Modular Approach to Treatment for Children with Anxiety, Depression, Trauma, and Conduct Problems (MATCH-ADTC).18
Regardless of whether individualized measures are used alone or in addition to standardized scales, the use of measures must be feasible. In fact, the more feasible a measure is to administer and score, the more often clinicians have discussions about scores with youth and their families.14 For children and their caregivers, the measures themselves should be brief and easy to complete, particularly when more than one type of measure is being used. This can help streamline the time needed to complete measures, which is a commonly expressed concern about implementing MBC.15 Brief measures can also ease scoring and interpretation for clinicians, who continue to experience increasing caseloads and administrative burden as the impacts of high clinical need and high workforce turnover persist. The recently published PAPERS framework 16 was developed using input from multiple stakeholders in behavioral health and provides criteria for identifying and rating measures on these qualities. Recommendations include ensuring that measures are readable at or below an 8th grade level, have clear cut-off scores and a streamlined scoring process, and use 10 or fewer items.
Clinical systems and processes could also be applied to enhance youth and family participation in MBC. Digital platforms are increasingly being used to help improve the feasibility of MBC by streamlining measure administration and scoring for clinicians. These measurement feedback systems also present opportunities to include youth and family engagement; for example, by using visual aids or graphs to display progress, or by easing the ability to browse and select measures with youth and caregivers. In addition, collaborative documentation is a patient-centered process that includes completing progress notes with clients during the clinical session. Collaborative documentation enhances transparency in behavioral health care and could be a framework through which youth and caregiver-identified metrics are routinely referenced, progress is discussed, and treatment planning occurs collaboratively.
Connecticut is a leader in evidence-based practices in children’s behavioral health and has a strong network of clinical providers who are experienced in administering standardized measures. The following recommendations are proposed to improve the implementation of MBC so that it jointly engages youth, families, and clinicians and builds upon efforts to improve children’s outcomes:
This Issue Brief was prepared by Alyssa Korell, Ph.D., and Jason Lang, Ph.D. For more information, visit www.chdi.org or Alyssa Korell at akorell@chdi.org.
Join CHDI's Email List to get our latest publications and updates on children's health and mental health issues.

