March 21, 2019

Sparked by research demonstrating the effectiveness and value of mobile crisis services, states and communities across the country are increasingly incorporating mobile crisis services into their continuum of care. Mobile crisis programs serve children in their homes and communities and divert children from high-end interventions (such as hospitalization or arrest) when a lower level of care is a safe and effective alternative. Mobile Crisis can also help reduce the number of visits to hospital emergency departments (ED), improve ED service delivery, and better meet the needs of children and families.
Connecticut’s Mobile Crisis Intervention Services (formerly known as EMPS) is available free of charge to all youth in the state under 18 years old, regardless of insurance type, system involvement, or other factors. Mobile Crisis is accessed through a single statewide call center, which deploys trained providers to the location where a crisis or other behavioral health need is occurring. Between State Fiscal Years 2011 and 2018, the program has expanded in volume by 54% while maintaining high service quality and demonstrating excellent child and family outcomes.
The Child Health and Development Institute of Connecticut, (CHDI) has worked with the Connecticut Department of Children and Families (DCF) since 2009 to ensure that Mobile Crisis delivers responsive, high quality care for children and families across the state. CHDI serves as the Mobile Crisis Performance Improvement Center (PIC), providing data analysis, monthly reporting, quality improvement, and professional development. In addition to the partnership between CHDI and DCF, achievement of positive results has been the result of strong collaborations among Mobile Crisis providers, 211-United Way, The CT Clearinghouse at Wheeler Clinic, Beacon Health Options, KJMB Solutions, family members and advocates, and other partners.
Highlights from the 2018* annual report demonstrate that Mobile Crisis Intervention Services are helping more children each year in their homes, schools, and communities. *State Fiscal Year (SFY) 2018 runs from July 1, 2017 to June 30, 2018

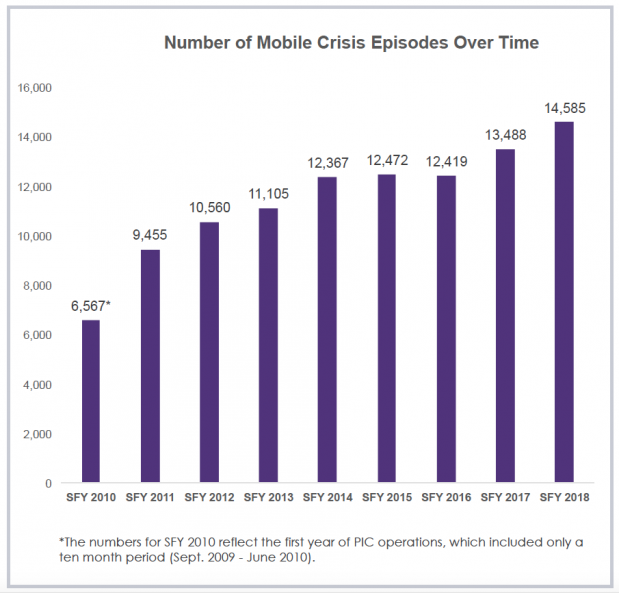
The number of Mobile Crisis episodes of care has increased by 54% since SFY 2011, the first full year of PIC data collection.
In SFY 2018, there were 14,585 Mobile Crisis episodes of care, 8% more than last year.
10,537 children were served by Mobile Crisis in SFY 2018.



In collaboration with the CT Clearinghouse at Wheeler Clinic, the PIC has delivered 284 trainings in the first eight years of PIC implementation. 596 Mobile Crisis staff members have been trained, helping to ensure clinicians deliver the highest quality care.

Connecticut’s Mobile Crisis program has continued to expand the number of children and families served over the last several years, while demonstrating excellent service quality and outcomes. As states increasingly recognize the value of mobile response services as a critical component of a comprehensive system of care for children with behavioral health needs, Connecticut’s Mobile Crisis service has been recognized as a national exemplary model. For the last several years, the National Technical Assistance Network for Children’s Behavioral Health, with funding from the Substance Abuse and Mental Health Administration (SAMHSA), has invited representatives from Connecticut to provide consultation to other states and communities interested in building or expanding their own mobile response service for children.
This Issue Brief was prepared by Aleece Kelly, Senior Data Analyst at CHDI. For more information on the Mobile Crisis Performance Improvement Center visit www.chdi.org or contact Kellie Randall at (860) 679- 8098 or randall@uchc.edu. For more information on Connecticut’s Mobile Crisis Intervention Services, visit www.empsct.org.
Join CHDI's Email List to get our latest publications and updates on children's health and mental health issues.