Share This Publication

Issue Brief 68: Building a Trauma-Informed Child Welfare System
May 16, 2019
Building a Trauma-Informed Child Welfare System
How CONCEPT Transformed Child Welfare to Improve Support for Children and Families Exposed to Trauma

Beginning in 2011, Connecticut launched a seven-year effort to transform the child welfare system to be trauma-informed. The majority of children in the child welfare system have been exposed to trauma, including physical abuse, sexual abuse, and chronic neglect, however emerging best practices for children exposed to trauma had not yet been implemented in Connecticut or nationally. A federal grant provided an opportunity for Connecticut to apply the concept of a trauma-informed approach to the state’s child welfare system. Today, Connecticut has made significant progress to ensure that children and families involved in the child welfare system are identified and have access to high-quality services. Connecticut is now one of the nation’s leading examples of a trauma-informed child welfare system.
The costs of maltreatment and trauma to children, families, and society at large are profound:
- Each year in the United States, more than 6 million referrals are made to the child welfare system and more than 600,000 of these children are determined to be substantiated victims of abuse or neglect.
- Among children in the child welfare system, 85% have been exposed to at least one potentially traumatic event and most have experienced multiple forms of trauma.
- Children exposed to trauma experience significantly higher rates of chronic health and mental health problems, impaired academic performance, and involvement with juvenile justice and adult criminal justice systems.
- The costs to society of children maltreated in a single year are $124 billion in future health care and social service costs.
Trauma-Informed Care Leads to Cost Savings and Better Outcomes for Children
As policymakers and providers have gained a better understanding of the adverse effects of trauma exposure and the benefits of treatment, there has been increasing support across child serving systems in Connecticut and nationally for early identification, intervention, and development of sustainable systems that incorporate a trauma-informed approach. The goal of a trauma-informed approach, also referred to as “trauma-informed care,” is to enhance systems to better understand, identify, and serve children exposed to trauma through prevention, training, screening, policy development, and access to evidence-based interventions.
Connecticut’s Approach to Addressing Trauma
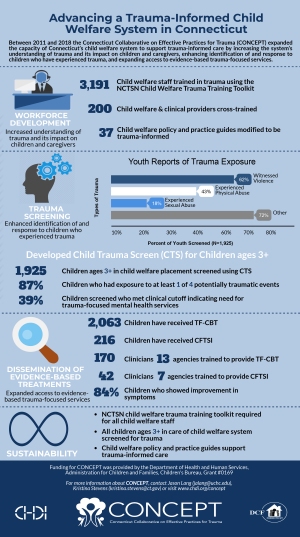
The Connecticut Department of Children and Families (DCF) was one of the first child welfare agencies in the country to incorporate trauma-informed care as a core strategy. In 2007, CHDI and DCF co-hosted the Connecticut Trauma Summit and disseminated Trauma-Focused-Cognitive Behavioral Therapy to 16 community-based agencies. Shortly after, DCF successfully applied for federal funding to transform the child welfare system to be trauma-informed. In 2011, the federal government awarded DCF with a $3.2 million grant, which ended in 2018, to develop the Connecticut Collaborative on Effective Practices for Trauma (CONCEPT). Support for CONCEPT was provided by the Department of Health and Human Services, Administration for Children and Families, Children’s Bureau, Grant #90CO1069. Partners included DCF, the Child Health and Development Institute (which served as the Coordinating Center), and The Consultation Center at Yale University (which served as the CONCEPT evaluator). The CONCEPT initiative has advanced four core components of a trauma-informed child welfare system:
- Workforce development: More than 3,100 DCF staff members have received comprehensive training in childhood trauma using the National Child Traumatic Stress Network’s (NCTSN) Child Welfare Trauma Training Toolkit. Training evaluations demonstrate significant improvements in DCF staff knowledge and practices concerning trauma. The training has now become required training for all new hires.
- Trauma screening: All children aged 3 and older who are placed into DCF care are now screened for trauma with the Child Trauma Screen (CTS). The CTS is an empirically supported 10-item screen that assesses trauma exposure and symptoms and can be administered by professionals in child welfare, juvenile justice, health, education, and behavioral health systems. More than 6,000 children, including 1,925 in child welfare, were screened through 2018 and referrals for specialty trauma-focused services are being made.
- Dissemination of evidence-based treatments: CONCEPT has helped to support training of more than 30 agencies and more than 800 clinicians to offer Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) and the Child and Family Traumatic Stress Intervention (CFTSI). These models add to the availability of trauma-focused evidence-based treatments in the state including Modular Approach to Therapy for Children with Anxiety, Depression, Trauma, and Conduct Problems (MATCH-ADTC), Cognitive Behavioral Intervention for Trauma in Schools (CBITS), and Attachment, Regulation, and Competency (ARC). More than 13,000 children across Connecticut have received these treatments, including many involved in the child welfare system. Evaluation outcomes indicate significant reductions in symptoms of post-traumatic stress and depression.
- Trauma-informed policy: The CONCEPT initiative has contributed to modifications of 37 DCF policies and practice guides to better address childhood trauma. For example, policies related to immigrant children, foster and adoptive services, and transgender youth and caregivers have been revised to ensure that DCF caseworkers consider children’s exposure to trauma and how it may affect their current functioning.
Recommendations for Advancing a Trauma-Informed Child Welfare System
Through CONCEPT, Connecticut has improved outcomes for children exposed to trauma by
leading enhancements in the areas of workforce development, screening, evidence-based
treatments, and policy changes. Recommendations for furthering a trauma-informed
approach in the child welfare system include:
- Expand collaboration between the child welfare, behavioral health, education, pediatrics, early care and education, juvenile justice, and other child-serving systems through cross-training and alignment of case plans, services, and data systems to move towards a statewide trauma-informed child health system. Existing statewide committees and workgroups focused on children’s health and behavioral health could be used to advance these recommendations.
- Incorporate assessments of a trauma-informed approach, achievable goals, and action steps into strategic planning for DCF and other state agencies.
- Expand trauma screening to enhance early access to services for all children, including children involved with the child welfare system who are not placed out-of-home, as well as for children who are not involved in the child welfare system (e.g., schools and primary care settings).
- Advance policy and reimbursement strategies that support dissemination and sustainability of evidence-based treatments, including models specifically designed for children under age 6.
- Support research to better understand the effects of a trauma informed approach on child and family outcomes.
Connecticut’s success in creating a trauma-informed child welfare system has spurred additional efforts across other child-serving systems including children’s mental health, early care and education, home visiting, education, juvenile justice, and health care. Efforts to implement a trauma-informed approach, as well as share trauma-focused services across these systems, have benefited from DCF’s leadership and the experiences and lessons learned through CONCEPT.
For more information, visit www.chdi.org, read CHDI’s IMPACT: Advancing Trauma-Informed Systems for Children, download the CONCEPT infographic, or contact Jason Lang (jalang@uchc.edu, 860-679-1550). Visit CHDI’s Evidence-Based Practice Directory to find sites offering some of the evidence-based practices available in Connecticut.
Download Issue Brief 68