Share This Publication

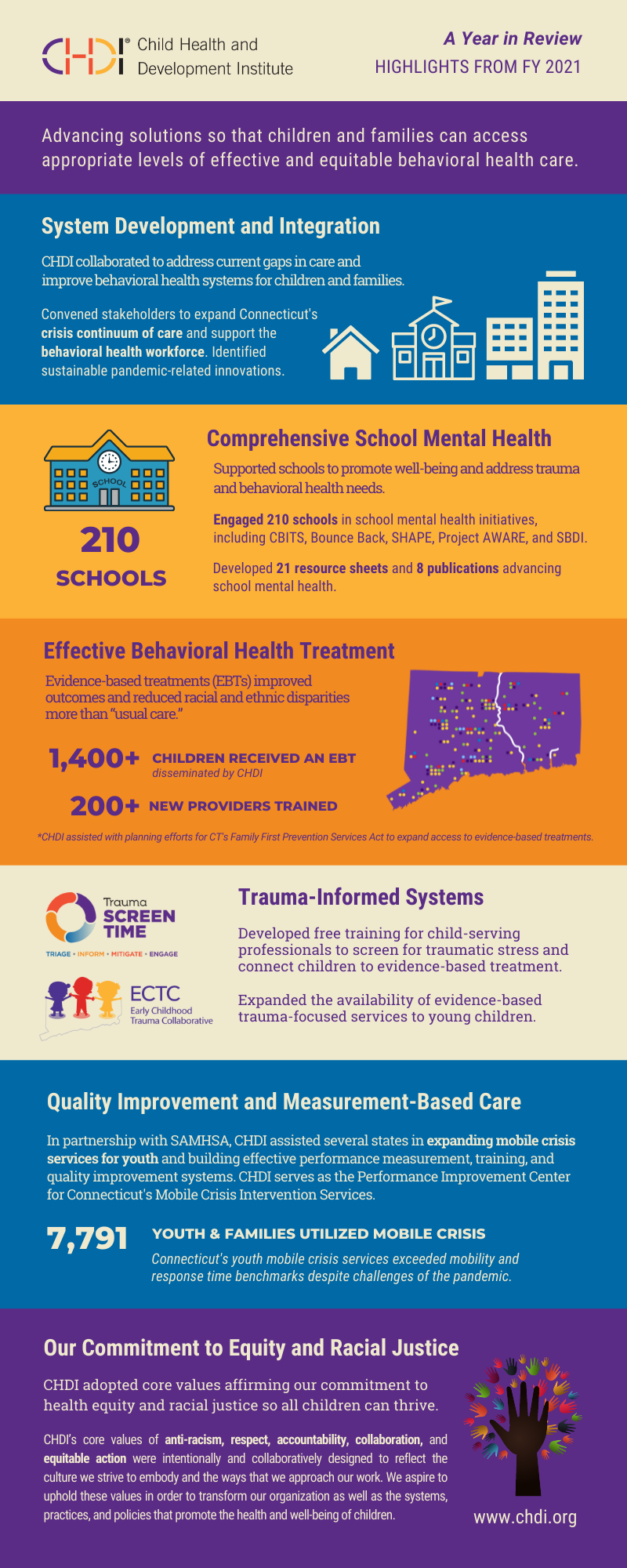
Reflections and Highlights from FY 2021
Letter from the President and CEO
Dear Colleagues,

This year has been especially challenging for children, families, providers, schools, and communities. The ongoing impact of the pandemic has significantly exacerbated behavioral health needs among children. Children from communities of color have been disproportionately impacted by adversity, inequities, and structural racism. A behavioral health system that was already under pressure has been strained even further by these unprecedented circumstances. With a renewed sense of urgency, CHDI and partners across the state are continuing to advocate for the systems, services, and professionals in place to address children's behavioral health and promote child well-being.
At CHDI, our efforts over the past year focused on improving care, addressing system gaps, and advancing solutions to address the enormous need for behavioral health services and supports. I am deeply grateful to our staff, our board of directors, and our many partners for collaborating to support children, families, and the providers that serve them. Together we overcame challenges and made progress toward our collective goal of building better systems, better policies, and better practices that result in better behavioral health for children.
Below are a few examples of our collaborative efforts to address the current crisis and improve children’s behavioral health and well-being.
- System development and integration. The current crisis has further strained the children’s behavioral health system and exposed gaps in services. This year, some of our most important work has been to convene policymakers, state agencies, stakeholders, and providers and develop immediate and long-term solutions. Our work to advance goals of the Behavioral Health Plan for Children and the State’s Connecting Children and Families to Care is leading to an expanded crisis continuum of care and is advancing efforts to recruit and retain a workforce capable of meeting the demand for behavioral health services.
- Comprehensive school mental health. COVID-19 had a profound impact on school staff and students this year. CHDI school mental health initiatives include SHAPE, the School-Based Diversion Initiative, CBITS and Bounce Back, and Project AWARE. CHDI shared resources and engaged 210 schools in initiatives to promote student and staff well-being and address students’ trauma and behavioral health needs. We produced a series of 21 resource sheets for supporting student mental health. We also partnered with the National Center on Youth Opportunity and Justice to publish a series of resources on school responder models.
- Dissemination of evidence-based treatments (EBT) and best practices. Children’s evidence-based mental health treatments and youth mobile crisis services contribute to a network of effective care and offer families and schools an alternative to hospital emergency rooms. This year, we trained 209 new clinicians virtually to deliver an evidence-based treatment, and more than 2,400 children received an evidence-based treatment disseminated by CHDI, including TF-CBT, MATCH-ADTC, CBITS, Bounce Back, ARC, and CPP. Evidence-based treatments were found to improve outcomes and reduce racial and ethnic disparities compared to “usual care.” We also assisted in planning efforts to implement the Family First Prevention Services Act, which will expand access to evidence-based treatments.
- Trauma-informed systems. This year, CHDI expanded our trauma-informed work to improve the early identification of children who have experienced traumatic stress and connect them to evidence-based treatments. Our Trauma ScreenTIME initiative (through the National Child Traumatic Stress Network) provides interactive online training for child-serving professionals to implement best practices for screening children for trauma. The training was pilot tested this year and will be available free for child-serving professionals early next year.
- Quality improvement and measurement-based care. CHDI continues to serve as the Performance Improvement Center for Mobile Crisis Intervention Services. Despite the many challenges presented by the pandemic, Mobile Crisis provided 10,542 episodes of care for 7,791 children and their families in SFY 2021. This year, in partnership with SAMHSA, we assisted several states in expanding mobile crisis services for youth and building effective performance measurement, training, and quality improvement systems.
As we reflect on the past year, we are encouraged by the commitment of our partners to address the challenges that lie ahead. As we look ahead to the coming year, we are dedicated to empowering policymakers with research and system innovations, supporting providers and educators with evidence-based and best practices, and sparking partnerships across sectors to solve problems and improve care. Our goal is to provide our partners with a bridge to better systems, better policy, and better practice leading to better behavioral health for children.
Best Wishes,
Jeffrey J. Vanderploeg, Ph.D.President and CEOChild Health and Development Institute